


Regulation, Insurance, Cost and the Decline of Healthcare Availability
Healthcare is a Special Trust
The narrative around healthcare accessibility for Americans begins with qualified data in 1873. Before that, healthcare was widely available though not as we know it now. Medical schools were numerous. But, mankind was not yet blessed with the scientific method. Medical practice in the “western tradition” was varied, with wisdom passed down through the ages in texts and through oral recitation. The basis for medicine was service to man. Even with such loose rules and primitive methodologies (by today’s standards) medicine was inextricably attached to ethics.
Doctors, especially good ones, have always been highly valued members of their communities. Many doctors in the US before modern medicine taught young doctors as a duty in their craft. The hippocratic oath tied ethics to the practice of medicine directly. The purpose of the wisdom was the betterment of the lives of fellow men. The promise made when taught the medical arts was that you took on a mantle of a very special trust between yourself and your fellow man.
Doctors from their beginnings in Ancient Greece had to promise to help when needed, to do only good with their knowledge, and never to do harm even through inaction. This contract was passed down from doctor to doctor for thousands of years standing the test of time – like few other principles ever did. The truth of righteous human interaction is manifest within the oath: Men who took on the knowledge of the body could do good with that knowledge or evil; the contract for gaining it was that they served their fellow men. This natural trust in our society is seemingly non-existent today.
The hippocratic oath and its many manifestations are now replaced by voluminous regulations. An examination of a century of healthcare decline in the United States along with the corresponding regulations that drove the industry’s evolution make a compelling illustration of how the fascist doctrines of licensure and currency controls are turned against the public trust. It is an especially compelling illustration because society is, again, trying to find solutions to the devastating economic trends that are making it impossible for people to get comprehensive access to doctors.
A Quick Aside on ‘Fascist Thought’
The purpose of this blog post is to cause discussion. The term ‘fascism’ is used in this post with a specific definition. Here fascism is referred to as the political philosophy of socialist central management though licensure and currency controls. Many pop-culture definitions of this word exist. They invoke imagery of death camps, jack boots, and cultural oppression. In the United States, the culture resisted fascism so its encroachment came more gradually like it did in England and France, but not like Germany or Italy whose adoptions were swift and terrifying, or in Spain or Russia where coups by Franco and Stalin brought fascism with immediate applications and more devastatingly evil impact.
Stalin had his committees pretending to be communist, handing favor of industry to his friends and developed a system of favoritism that would dominate the Soviet economy until it’s realignment. Germany made wider concessions granting companies like Volkswagen, BMW, and Mercedes into pseudo-competing models. In the US fascist economic policy took the form of immigration laws, wage controls, economic development initiatives, and then regulatory committees. The difference in how this philosophy took hold was one of speed and penetration. The specific economic strategies, however share one specific common thread: Government licensure and currency control.
This socialist economic strategy is the definition of the word ‘fascist’ that is used here. The reader may object because of the emotional impact of the word. I do not blame them. Their emotions should be heightened. The economic principles of fascism are devastating to both the economy and the society that adopts them. Fascist strategies lend themselves to out-of-control feedback loops and authoritarianism. The faster the adoption, the stronger the application of violence was manifest in the societies.
The emotional reaction the word evokes is valid, however cowing to that emotionalism has caused us to miss the evil pervasive in our own society – to miss the actual jackboots that inspire “Black Lives Matter”, and the actual concentration camps that make us the most imprisoned of all nations. We have a truth to face as Americans if we are ever to have access to healthcare, much less effective education and a thriving economy in general. We must acknowledge that we adopted fascist policies in the 20th century, that we are in denial of this fact, and that when we turn to face it, we will become much more healthy and happy as a people.
We are in a transitional time. The generations for which this word is evocative are largely passed on, and a better understanding of ‘fascism’ is resolving as the mists of denial drift off into time. Younger generations starting with the baby boomers increasingly understood the brainwashing their parents and grandparents were afflicted with in this age. For us, the word ‘fascist’ is increasingly important as a guide away from the failures of some past generations.
The United States was fortunate to have had a strong tradition of individual rights. When fascism was running rampant in the world it only got “half-way” in the US. It is also unwinding here and elsewhere where civil rights still exist nominally. Medical care’s history in the US is one that unmistakably follows the fascist model. The mistakes we made over 100 years ago in following the fascist model require a defining word – a pin in the map. That pin in the map, identifying that philosophy and the naive time in which it flourished, in this work’s context, is the specific definition of “fascist thought” used here.
I propose that understanding this model is the key to once again having access to medicine for everyone in society. It will not be done through socialist and fascist means. Those strategies have failed us. Those systems rely on a shortage of supply, and they keep the supply short to maintain themselves. We need to recognize that “healthcare” is about a patient and their doctor. Anyone else trying to insert themselves in that relationship with force is going to destroy the necessary trust that medicine demands. Any institution that inserts itself in there with law will destroy healthcare in all aspects.
Modern Medicine
Modern medicine began in the US when Johns Hopkins established what would become the model hospital in 1876. Doctors were plentiful for the most part. Hospitals concentrated specialized care and increased access to technology. Healthcare at the turn of the twentieth century was very affordable. The cost of a doctor visit was about one dollar, or about $20 in today’s money. Aside: My co-pay is twice that.
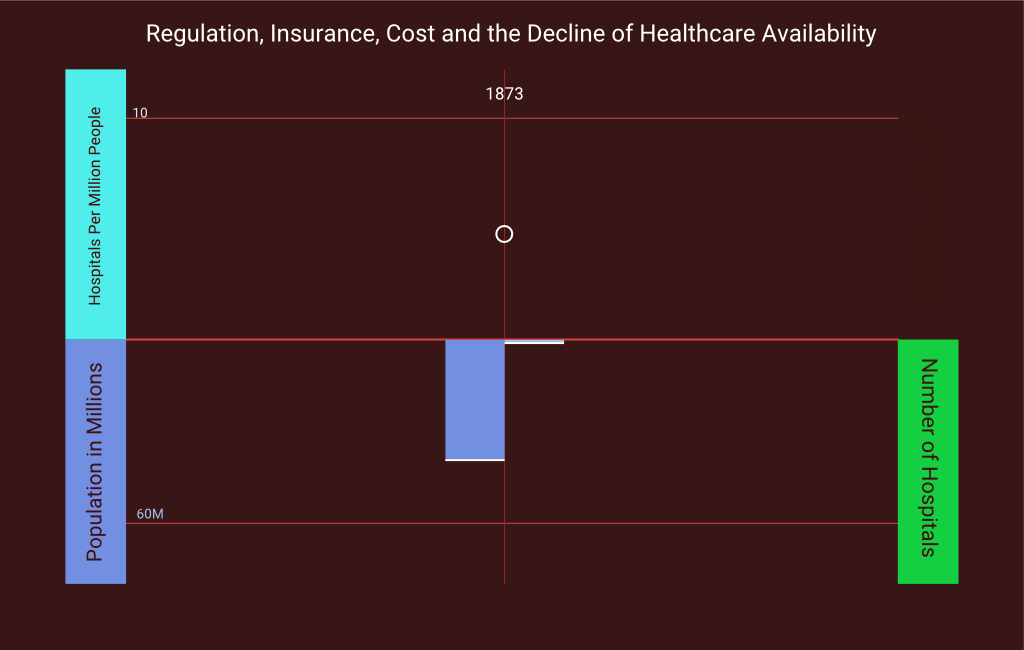
The application of the scientific method on medical research brought great advances to medicine; all of them good. Once mankind adopted science, the study of the human body and how to mend and strengthen it took off. By 1904 there were over 4300 hospitals in the US following Johns Hopkins model. There were over 52 hospitals per million people in the US. This would be the high point of medical accessibility for Americans. The study of medicine was flourishing and that attracted the attentions of men who had learned a new game: Using government and regulation to narrow markets into the hands of the politically connected.
The AMA’s Growing Relationship with Government
An organization emerged in the nineteenth century with a noble purpose. The American Medical Association created advisory statements on medical practices. Along with several other organizations they advised people about what was good medicine and what was snake oil. The success of their education efforts, however, took on a dark and perverse cast, one shaped by the raise of fascist economic ideology. Early on they started to adopt the unwholesome tactic of seeking the use of law to regulate medicine. Citing “quackery” they began advising the state to adopt laws requiring the registration of births, deaths and even marriages. They pushed forward national laws regarding quarantine procedures, and compulsory vaccinations.
While a majority of the educational work the AMA did was very valuable to the populace, they began to be affected by their relationship to the legislative process. Their educational materials and their focus narrowed to systems that were easy to apply at massive scales. Instead of being guided by principles, the AMA began codifying rules to keep doctors and the profession of medicine strictly inside the narrow confines of what could be enforced. Instead of advising and educating – instead of informing and empowering – they began directing and dictating.

In 1910 the AMA published a report with funding from the Carnegie Melon Foundation. The Flechner Report claimed that most medical schools where “diploma mills” and the AMA began calling for more control on the spreading of medical knowledge and the restriction of its practice. By 1912 they had secured themselves as the authority for medical law and licensing in the states. More than half of the medical schools in the US were closed and many hospitals, closed and quickly changed ownership or administration to conform to the AMA’s unilateral licensing procedures. The accessibility to healthcare for Americans began a steep century long decline we have not yet recovered from.
By 1925, fascist thought was gaining popularity. Institutions like the Federal Reserve and the AMA who were not government, and not private, but something else… something that could only exist in autocracy… began using their legislatively granted economic muscle to manipulate the populace. Government regulation started becoming a popular way of dealing with social problems and long lived organizations focused on philanthropy began to be subsumed by committees with political favor.
Calvin Coolidge began allowing medical patents to be issued. Previous to this and previous to the AMA’s demi-government control, it was unthinkable for doctors to deny medical help to people in need. Now, with the threat of criminal prosecution, and loss of career, doctors were restricted in how they could deliver that service. It had once been unthinkable to use intellectual property to restrict medical care. Suddenly men could withhold access to even the idea of a procedure or device and the government itself became an agent of withholding medical care for the unprincipled concept of patent and license.
The Twentieth Century and the Rise of Fascism
Through the beginning of the twentieth century and the rise of fascism, the AMA gathered tremendous power. They had become the one and only source for license to become a doctor. By 1945, fascism in the US was in it’s post-war heyday. After World War 2 there was not a single industry that was not significantly licensed through political favor. The AMA had already moved into inspecting food and had elevated psychiatry to the level that the practice was embedded into criminal and family courts. It had established state sponsored grant programs that directed medical research into fewer hands. They had even pushed for alcohol limits and tests for drunken drivers.

It is important to note that this pervasive evil was not born and brought by evil men. None of these pursuits were themselves evil in intent, but in implementation in always using government to enact these social solutions. The problems were real, but because of the AMA’s power over the life and death of every American, they were able to make society turn to law enforcement to combat misfortune and stupidity. The natural evil that was once supposed to be contained in government – the authority to do violence – was released from the burden of the Republic’s constitutional limitations.
Problems that had once been solving themselves through advancements in communication and technology were now being directed by groups that did not tolerate any deviation from their dictates – dictates that often seemed ambiguous because they were politically motivated, not crafted for the health or welfare of people. Safe and effective folk remedies known to healers for centuries were made illegal. The neighborhood wise-women and others who once rendered first aid, were jailed for practicing medicine. Those who tried to defend themselves in the courts or by addressing the public were targeted with prejudice.
The government enforced the AMA’s program in the market ruthlessly. The progress of medical advancement in the once burgeoning scientific community began to slow. Medicine had its voice and scientific innovation reduced to the confines of a few men with a strict perspective on health care. Whole schools of medicine had been wiped out or sent underground. The number of hospitals grew in those decades, but not enough compared to the population. The number of hospitals in the US grew by only 25% in these 30-40 years of increasing AMA control but the population grew much faster increasing 75% in that span. The ratio of hospitals to people dropped to a little more than 42 hospitals per million as a nominal rate. Government research facilities and veterans hospitals had been promoted more than civilian ones in the new economy. These hospitals were not available to the public, thus the meaningful rate of accessibility was only 36.5 hospitals per million.
Medical schools were restricted on how many graduates they could produce a year. The healers of the neighborhood could no longer treat minor health issues with advice. Even a headache or a cut required a license to give advice or aid. The World Wars had brought with it the advent of government hospitals, primarily serving veterans – poorly. Access to healthcare had hit a low, and people were outraged. Declines in access once blamed on war efforts and economic depression were painful to the people. Before, Americans had great access to doctors. The Roosevelt administration, a great progressive friend to the AMA moved forward legislation to solve the problem with more regulation and privileges for the elites whom would fill their committees.
The New Deal’s Special Deal for Insurance
Medical insurance was given privileges in the post-war economy in 1945 with the McCarran-Reguson Act. The industry immediately began to consolidate into a few hands of the politically connected. The next year The Hospital Survey and Construction Act moved government into every medical provider by providing funding, with very heavy strings and bloated administrative requirements. All of it overseen by the AMA and their political allies which aimed at control, not access.
From 1946 to 1956 the United States economy was transformed in terms of medical care but not necessarily in a good way. Health insurance, firmly attached to government favor and immune from antitrust, took over health care and the entire industry began to reduce and narrow on all levels of provider-ship.
Consolidations backed by government grants and special license from the AMA put pharmaceutical supply, medical equipment, facilities, and the very supply of doctors and nurses into their very small circles of friends. The very model of fascism, narrow licensure, autocratic destruction of competing views, burdensome requirements selectively enforced against political enemies, and public shaming of dissenters dominated healthcare. The entire industry was regulated into a cartel, and protected from antitrust.
Health insurance became the dominant source of health access, and the once tiny, unwanted industry was thrust into the economy as job benefits with massive tax incentives. So ubiquitous was the domination and so rapid the takeover, that within only about 10 years, the people of the United States went from 9% having insurance to 75% in 1956. It was not long before the rest of the people, the uninsured, could not even get a check-up or see a doctor for a routine emergency need like a broken bone.
Cost Plus Profit Models and Vertical Integration
The introduction of insurance did not make the industry, nor the American people more healthy. The number of hospitals to people began to decline further. The price of healthcare as expressed by the “Medical Care Price Index” began to outpace the Consumer Price index marginally but immediately. Medical access became, in very short time, a government mandated privilege only to the middle class with 25% or more of the populace not able to get access except through charity. Minorities, not surprisingly, were the ones primarily excluded from jobs that brought health care insurance.

In 1965, Medicare and Medicaid were passed to make up the healthcare gap, and acted to further isolate racial groups into second class citizens. The same people who created the gap, now administered massive government funds meant to provide for the portion of the populace who did not have insurance and were priced out of seeing a doctor. Access continued to decline with falling rates of hospital construction and in the numbers of new doctors graduating.
Medicare further drove a particular evil called cost plus. Very popular in the age of fascism, this model only existed within markets completely controlled. Presented as a control on costs, it served the opposite effect. The idea is that insurance companies had to restrict their profits by making only a small percentage in profit above their costs. The same model was used pervasively for government contracts and other industries where the fascist doctrine of government license was applied.
The politically connected would generate regulatory requirements through their lobbying that matched their already in place procedures. Their rivals would be destroyed, unable to absorb the costs of changing their processes to match the overly specific and burdensome ones the elites dictated. Then once their competition was eliminated, they could dictate costs and profits without competition or restraint. Cost plus profit models, backed by regulations, allowed elites to monopolize the entire vertical market in healthcare. The medical industry was suddenly dominated by holding companies that owned both hospitals and medical suppliers, specialized middle-men, that would negotiate massive contracts between conglomerates. Deals that in any other industry would be recognized as illegal collusion from a position of legislated privilege. Indeed, in most other industries, in government contracts especially, the cost plus model has been made illegal. But in healthcare it persists, and it would literally take an act of congress to change it.
By 1975 the market in health care was so constricted that the ratio of hospitals fell to under 33 per million people. Making matter worse, the number of hospitals we count include government hospitals and for profit hospitals that provide elite and elective surgeries, not healthcare. The number of not-for-profit hospitals available to the public gives a realistic number of only 26 hospitals per million.
Responding to the crisis that his political sponsors helped create, Nixon passed more laws and executive orders implementing the worst regulations left dormant, and thought unconstitutional in the Hospital Survey and Construction Act authorizing regulators to demand mountains of documents and requirements from hospitals. All of the requirements meant needing to hire more licensed staff that did paperwork, not healthcare and to purchase new equipment; equipment supplied by patent based businesses owned the same people who owned the hospitals and the insurance companies.
A Decade of Hospital Failures
The medical industry in the United States in just 25 years following the passage of the New Deal measures became extremely narrow. Every aspect of medicine was consolidated into very few hands. Immunity from anti-trust and armed with protectionist regulations elites in the medical industry used the political influence and the draconian regulations to destroy businesses, and then take over the assets in bankruptcy.
Following the passage of Medicare and Nixon’s implementation of regulations, hospitals began failing in large numbers. Emergency rooms, once a model of social advancement in medicine, began to evaporate. Hospitals once run by community benefit organizations were taken over by the corporations that drove the regulations that sent hospitals into receivership. Boards of Directors were no longer members of the community whom had a vested interest in philanthropy. They were replaced by men who demanded profitability for the mega-corporate holding companies that owned them.
Profitability did not mean the hospital needed to show a profit. Indeed most hospitals were regulated into a non-profit status. The profit was instead realized in the narrowing of medical supplies. Here the elites had the political clout to dictate patents and regulations, but were also unfettered with price controls. These men, taking over the failing not-for-profit hospitals all began paying incredible and unreasonable amounts of money to their unregulated business partners. A modern day illustration of this effect is the now famous $700 bag of saline. It does not cost anywhere near $700 to make, store and distribute sterilized salt water in non-allergenic bags. Regulations however make it so that only a small number of people have license to make salt water in a bag, and the medical cartel makes sure that the hospitals only buy from a supplier that they also own.

The number of hospitals went into free fall and the price of medical providers shot through the roof. By 1986 the medical profession was in a shambles compared to the golden era of free market medicine. Even though the populous now had 86% access to health insurance, access itself was in the toilet. The population continued to rise but the number of hospitals dropped. The ratio was at only 22.5 hospitals per million people at the nominal rate. Though lower than imaginable already that number is off by quite a bit. Massive government grants for research, and swelling needs for treating veterans inflated government hospitals to record numbers.
Government hospitals for limited use or research swelled and elective medical grew while healthcare for the people languished. In 1986 only 3420 general not-for-profit hospitals remained in the US making the ratio for access only 18.3 hospitals per million. More people had access to health care from insurance, or so you would think, but not so… Now there were waiting lists and approval procedures that lasted long enough that the afflicted would sometimes just die before getting treated. The level of care had disappeared, treatment time was reduced to an order of magnitude less, but costs skyrocketed. The perpetrators of the scam were all privileged men, politically connected and protected by law from any liability by the very regulations purported to prevent the abuse.
A Monopolized Market in Healthcare
The cost of healthcare was out of reach even for the insured. The MCPI became double the CPI. If you didn’t have insurance, you could not afford to catch even the flu; copays for something big were catastrophic and the doctors and nurses treated you like complete shit spending far more time running you in procedural circles than treating your ailments.
Today the disparity continues to get worse, and Obamacare is certainly contributing the systemic failure by driving insurance into a mandatory model. The cost of healthcare in the MCPI is still more than double CPI meaning that inflation in healthcare has been double the rate of the rest of the consumer economy for over 30 years. Today, a stay at a hospital for one night can cost 2 months of gross income for a median income family.

Never in the history of man, have doctors and healthcare been so corrupt. The twentieth century brought us modern medicine, but also brought us crushingly immoral social and political strategies. The emotional sensitivity of healthcare access makes it ironically hard to fix. The strategies of autocratic rule rely on fear, and when the matter is one of life and death, the emotion is very easy to invoke.
The problems of healthcare are obvious even to the most privileged in society. All but the most politically connected feel or have long felt their access and quality of care slip, even in the face of miraculous technological advancement. Most however are feeling a massive pinch. Few are alive that remember when healthcare was freely available and when there were emergency rooms plentiful in urban areas. Over a century, law guided by fascism eroded healthcare little by little. Each generation that passed had less access to doctors than the previous.
If we are going to solve the problem of healthcare access as a society, we must face the plain truth. Our system of regulation has not made healthcare better. With the decline of access so easily demonstrated, with the costs skyrocketing the way they are, with such easy demonstrations of how the foundation of the system is corrupt – one has to wonder why we have not fixed the problem yet. Why do we hold onto such a draconian system of healthcare still? Why are the only solutions discussed, ones that further compound the same failures that caused them?
I believe that it is the delusion that also keeps us from recognizing fascism within the policies formed in the 20th century. We need to embrace the failures of those now gone generations, face the fascist policies they naively allowed into our society, and set healthcare straight by undoing their destructive influence.
An Invitation to Expand
This narrative and the infographic that accompanies it were inspired by an article from the Mises Institute and several other sources of data. As a personal note, I offer many assertions that I recognize are not supported with evidence in this blog post. Many of them are addressed in these below links. Others, like the ambiguous definition of “fascism” I use in a context I hope is made clear as illustrative. To produce a schollarly work on this subject is beyond my intent. To spark discussion and to promote a more sophiticated understanding of the market forces involved in the modern medical crisis.
I invite the reader to research and to comment on any assertions that they can support or that they can find contradictory evidence to. This work may one day be fleshed into a format more fitting of the dense amount of information that supports it claims. I specifically offer it in it’s raw form for the reader to muse over, and to research their own understanding of how regulatory forces have undermined medical access.
How Government Regulations Made Healthcare So Expensive
https://mises.org/blog/how-government-regulations-made-healthcare-so-expensive
Income, Poverty, and Health Insurance Coverage in the United States: 2010 / Current Population Reports – Consumer Income; By Carmen DeNavas-Walt, Bernadette D. Proctor, Jessica C. Smith
http://www.census.gov/prod/2011pubs/p60-239.pdf
Hospitals: Origin, Organization, and Performance
http://www.jblearning.com/samples/0763749745/49745_Ch03.pdf
Hospitals By Ownership Type
The Kaiser Foundation
How to Charge $546 for Six Liters of Saltwater
By AUG. 25, 2013



